


One in three babies born in the United States today arrives via cesarean section (C-section birth). Globally, C-section rates have surged in both high-income and developing nations, and while this surgical intervention has saved countless lives, a growing body of evidence asks us to look more carefully at what a baby may miss when born this way.
A landmark 2026 systematic review published in the World Journal of Clinical Pediatrics, synthesizing 75 studies and data from millions of births across multiple continents, makes one thing unmistakably clear: the way a baby is born has measurable, sometimes lasting, consequences for the gastrointestinal (GI) tract. The review, led by Al-Beltagi and colleagues, evaluated both short-term disturbances such as colic, reflux, and constipation, and long-term conditions including inflammatory bowel disease (IBD), food allergies, and celiac disease.
“As a physician who has spent years exploring the root causes of chronic illness, and as a patient who has lived through my own gut health journey with Crohn’s disease, I can tell you without hesitation: the very first hours of your baby’s life lay a foundation that can shape their health for decades. How your baby enters the world matters more than most parents, and even most doctors, realize.” — Dr. Jill Carnahan, MD
In functional medicine, we ask the question most conventional medicine skips: WHY is this happening? The answer, woven through nearly every study in this review, is the gut microbiome.
Important note: C-section delivery is often medically necessary and genuinely life-saving. This article is not intended to cause guilt or alarm in mothers who have had C-sections. The goal is empowerment through information, so that families who know this risk can take proactive steps. Every birth story is unique, and healing the gut microbiome is absolutely possible.
Part 1: Why the Mode of Birth Is a Gut Health Story
The Birth Canal Is a Microbial Initiation Ritual
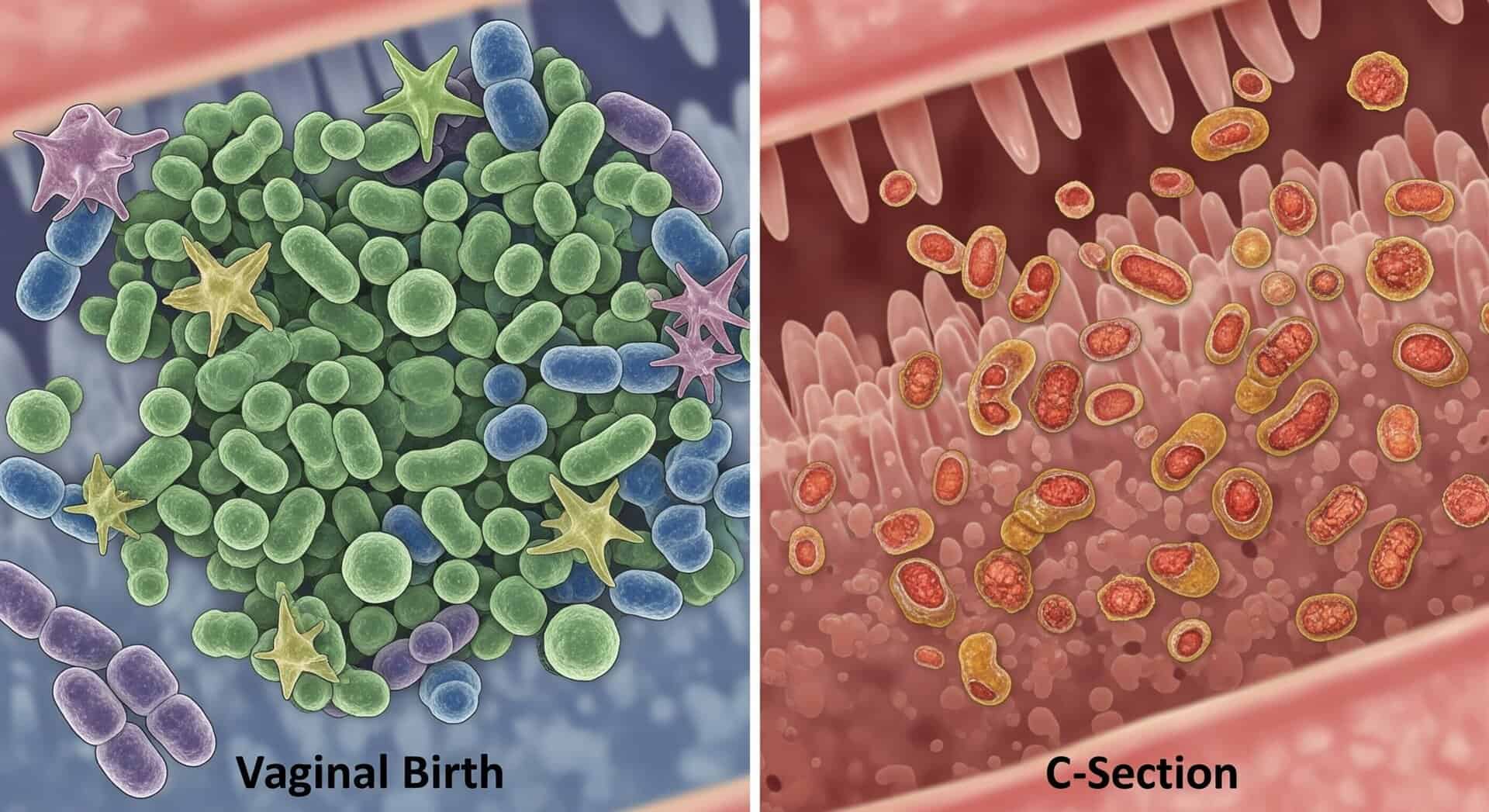
When a baby travels through the vaginal canal, something remarkable happens. The newborn is bathed in maternal vaginal and fecal microbiota, seeding the infant gut with foundational species: Lactobacillus, Bifidobacterium, and Bacteroides. These are not random bacteria. They are keystone species that:
- Digest human milk oligosaccharides (the complex sugars in breast milk that babies cannot break down alone)
- Produce short-chain fatty acids (SCFAs) that nourish gut lining cells
- Educate the developing immune system
- Build mucosal barrier integrity
- Create an anti-inflammatory gut environment
C-section-born infants, by contrast, bypass this exposure entirely. Instead of being colonized by beneficial maternal microbes, they are colonized by whatever microbes exist in the hospital environment and on skin surfaces: Staphylococcus, Klebsiella, Enterococcus, and Clostridium species. This foundational difference sets off a cascade of consequences that can ripple for months, years, or even decades.
The Statistics Are Striking
The review draws on data from multiple large-scale cohorts. From a Danish registry of 2.1 million individuals followed for up to 35 years, to a Korean national cohort, to the UK Baby Biome Study, the research consistently documents:
- Reduced microbial diversity in C-section-born infants
- Delayed colonization by Bifidobacterium and Bacteroides
- Increased colonization by opportunistic pathogens
- Differences in microbiome composition that can persist beyond 12 months
As a clinician who regularly sees adults with complex chronic conditions tracing their roots back to early-life gut disruptions, these numbers are not abstract. They represent real people sitting across from me in my practice, trying to understand why their bodies have been so difficult to heal.
Part 2: Short-Term Consequences of C-Section Birth
The immediate postnatal months are a window of extraordinary vulnerability and opportunity. C-section-born infants face a significantly higher burden of functional GI disorders (FGIDs) in this period, and the evidence is robust.
Infantile Colic
Six studies in this systematic review examined colic in C-section versus vaginally delivered infants. The findings were consistent. A 2019 prospective cohort study by Salvatore and colleagues involving 934 infants found that infantile colic affected 47.4% of infants overall, with C-section delivery carrying a relative risk of 1.23 (95% CI: 1.07-1.40; P = 0.003). That is nearly a quarter more risk.
In a large retrospective study of 988 preterm infants, 45.4% had infantile colic, and C-section was a significant risk factor across all functional GI disorder categories (P < 0.001). Even more telling: C-section-born infants who were also given antibiotics and formula-fed faced the highest risk of all.
Why? Because colic, in many cases, is not a mystery. It is an inflammatory event. Research shows that C-section infants display elevated fecal calprotectin, a biomarker of intestinal inflammation, even when they do not have colic. The gut is inflamed. The microbiome is disrupted. And a colicky, inconsolable baby is often a baby whose gut is trying to communicate that something is wrong at a foundational level.
Gastroesophageal Reflux (GER/GERD)
In an extraordinary population-based cohort study of 869,188 infants by Dahlen and colleagues, infants born via C-section were significantly more likely to be diagnosed with GER or GERD: 37.2% compared to 28.4% in vaginally delivered infants. Multivariate analysis confirmed C-section as a significant independent risk factor with an adjusted odds ratio of 1.13 (95% CI: 1.08-1.78).
The microbiome connection is direct. Research by Pantazi and colleagues documented that infants with GER had significantly reduced levels of Lactobacillus and Bifidobacterium (the acidifying, protective flora) and increased levels of Escherichia coli and Klebsiella. This microbial pattern, strongly correlated with C-section birth, is the likely physiological driver of reflux pathophysiology.
In my functional medicine practice, reflux in infants is rarely just a matter of antacids. It is a signal that the gut ecology is off, that the delicate acid-base balance of the early intestinal environment has been disturbed. When I see a C-section baby on a proton pump inhibitor at three months old, I want to ask: have we addressed the microbiome?

Functional Constipation
The evidence here is more nuanced but still significant. The Japan Environment and Children’s Study, one of the largest datasets ever assembled on this question involving over 71,000 children, found a statistically significant modest increase in functional constipation at age 3 among C-section-delivered children (13.1% vs. 12.1%; adjusted odds ratio = 1.064). While the absolute difference is small, when applied across a population of millions, it becomes consequential.
Bi and colleagues, studying 988 preterm infants, found a much more dramatic result: 19.2% developed constipation in the first year, with C-section as a significant risk factor (P < 0.001), compounded by antibiotic exposure and formula feeding.
One particularly interesting finding: infants given probiotics in the Ziętek 2024 study showed an unexpected increase in constipation at 3 months. This underscores a critical functional medicine principle. Not all probiotics are created equal. Strain specificity matters enormously, and blanket probiotic use without understanding the individual microbiome landscape can sometimes backfire.
Clinical note: Probiotics vary enormously by strain, dose, and timing. The unexpected constipation finding in one study likely reflects strain-specific effects rather than a problem with probiotics as a category. Clinicians and parents should work with knowledgeable practitioners to select evidence-based strains appropriate for the infant’s age, delivery mode, and feeding method.
Part 3: Long-Term GI Consequences That Extend Into Childhood and Beyond
Perhaps the most sobering section of this systematic review involves the long-term immune-mediated GI conditions. The gut microbiome formed in the first weeks of life does not merely affect digestion. It trains the immune system. When that training is disrupted at birth, the downstream consequences can manifest years later as chronic disease.
Inflammatory Bowel Disease (IBD): Crohn’s Disease and Ulcerative Colitis
The evidence for an association between C-section and IBD is genuinely mixed, but the quality studies that DO show an association are hard to dismiss. Bager and colleagues analyzed a Danish cohort of 2.1 million individuals followed for up to 35 years and found that C-section was associated with a moderate increase in IBD risk before age 15 (incidence rate ratio = 1.29; 95% CI: 1.11-1.49). A Swedish cohort of 1.1 million individuals specifically linked C-section to elevated Crohn’s disease risk with an adjusted hazard ratio of 1.14 (95% CI: 1.02-1.27).
Critically, the association was stronger for Crohn’s disease than for ulcerative colitis, and stronger for elective C-sections than emergency ones. This distinction is biologically meaningful. Elective C-sections, by definition, occur before labor. This means the infant misses not only vaginal microbial exposure but also the hormonal and physiological cascade of labor itself, including oxytocin release, stress hormone priming, and the physical compression that helps expel fluid from newborn lungs and GI tract.
I have Crohn’s disease myself. I know intimately what it means to live with a gut that turns against itself. When I see data suggesting that a modifiable decision at birth (choosing an elective C-section without medical indication) may increase a child’s risk of Crohn’s disease, it is not academic. It is personal. And it should prompt us to counsel expecting parents with both honesty and compassion.
Not all studies agree. Robust datasets from Canada, the UK, and Germany found no significant association between C-section and IBD. The truth appears to be that C-section is one contributor in a multifactorial pathway, not a single deterministic cause.
Celiac Disease
A large Italian multicenter study found C-section in 40% of children diagnosed with celiac disease, higher than the general population rate. A Swedish matched case-control study of nearly 12,000 celiac cases found a significant association specifically with elective C-section (adjusted odds ratio = 1.15). Yet large cohort studies from Canada, Norway, and Denmark found no significant link.
The review’s conclusion on celiac disease is measured and honest: C-section may act as one of several early-life exposures that influence immune and gut development, but it is not sufficient as a standalone risk factor. Genetic predisposition (especially HLA genotype), antibiotic exposure, timing of gluten introduction, and breastfeeding practices all play roles that likely outweigh delivery mode alone.
Food Allergies and Cow’s Milk Protein Allergy (CMPA)
Here the evidence is more consistent, and the effect sizes are larger. Multiple large cohort studies reported significant associations between C-section delivery and food allergy risk. A Greek case-control study found C-section associated with more than a threefold increase in food allergy risk (odds ratio: 3.15), especially when combined with parental atopy. A Norwegian study found a sevenfold increase in food allergy risk in C-section-born children of allergic mothers. A Swedish population-based cohort of over one million children found a hazard ratio of 1.21 for food allergy.
For CMPA specifically, the risk compounding is striking. A Spanish retrospective study found that C-section combined with formula feeding in the hospital setting carried an odds ratio of 11.82 for IgE-mediated cow’s milk protein allergy. Eleven-fold. When we consider that CMPA is the most common food allergy in infancy, affecting up to 3% of children globally, these numbers represent enormous suffering and healthcare burden that may be substantially preventable.
The protective factor that kept appearing across study after study? Breastfeeding. Exclusive breastfeeding consistently buffered the allergy risk in C-section-born infants. And targeted probiotic supplementation, particularly perinatal supplementation with specific strains, reduced IgE-associated allergy incidence in C-section-born infants with an odds ratio of 0.47 in the Kuitunen 2009 Finland study. That is a 53% reduction in IgE-associated allergy with carefully selected probiotics.
Research note: Not all studies confirm the food allergy association. Large Australian, Taiwanese, and Japanese cohort studies found no significant link between C-section and food allergy. Geographic variability, differences in genetic background, baseline microbiota composition, diet, and diagnostic criteria all influence results. The association appears strongest when C-section is combined with formula feeding and antibiotic exposure.
Part 4: What You Can Do — Evidence-Based Strategies for Gut Microbiome Restoration
This is where functional medicine shines. The research is not simply a story of risk. It is a roadmap for intervention. The gut microbiome is dynamic. It responds to inputs. And while we cannot change how a baby was born, we absolutely can influence where their microbiome goes from here.
1. Breastfeed If at All Possible
The single most powerful, evidence-based intervention for restoring microbial balance in C-section-born infants is breastfeeding. Human breast milk contains human milk oligosaccharides (HMOs) that selectively feed Bifidobacterium species. Breastfed C-section infants in multiple studies showed significantly better microbial recovery, approaching the diversity of vaginally delivered infants within weeks to months. Breastfeeding showed synergistic effects with probiotics as well. If breastfeeding is not possible, donor human milk is the next best option.
2. Targeted Probiotic and Synbiotic Supplementation
Synbiotics (combinations of specific probiotic strains with prebiotic fibers) showed the most sustained and significant effects on microbiota restoration in C-section infants across this review. Formulations containing Bifidobacterium breve M-16V with scGOS/LcFOS oligosaccharides promoted early Bifidobacterium colonization, lowered fecal pH, and emulated the gut profiles of breastfed or vaginally delivered infants with effects persisting up to 12 months.
Other strains with evidence in C-section infants include:
- Lactobacillus reuteri (for reducing colic and reflux)
- Bifidobacterium bifidum (sustained improvement in microbial diversity at 12 months)
- Lactobacillus rhamnosus GG (allergy prevention when used perinatally)
- Multi-strain combinations including Bifidobacterium breve and Lactobacillus rhamnosus
At Dr. Jill Health, we carry targeted probiotic formulations designed to support the developing infant and childhood microbiome. Visit drjillhealth.com to explore options and work with a knowledgeable practitioner for personalized guidance.
3. Minimize Unnecessary Antibiotic Exposure
Intrapartum antibiotics are standard in C-section deliveries for infection prevention, and this is appropriate. But the research is unambiguous that additional antibiotic exposure (including neonatal antibiotics for non-urgent indications) compounds the microbiome disruption significantly. In every study examining modifiers, antibiotic exposure amplified the risks of colic, reflux, constipation, and long-term immune dysregulation. If your C-section baby requires antibiotic treatment, advocate for concurrent probiotic support and microbiome restoration strategies.
4. Skin-to-Skin Contact and Rooming-In
While skin-to-skin contact does not directly transfer vaginal microbiota, it powerfully supports the hormonal and bonding environment disrupted by surgical birth. Oxytocin release, facilitated by skin-to-skin contact, supports neonatal gut motility and the early initiation of breastfeeding. Multiple studies in this review noted maternal psychological health (particularly postpartum depression) as a modifier of infant GI outcomes. A mother who is supported, bonded, and able to breastfeed is giving her baby the best possible start, regardless of how the birth occurred.
5. Consider Vaginal Seeding (with Informed Guidance)
Vaginal seeding (the practice of swabbing C-section babies with maternal vaginal fluid at birth) was investigated in multiple studies in this review. The results were mixed but generally showed partial microbiome restoration, particularly in skin and oral sites, with some gut colonization improvements. The swabbing technique appeared more effective than oral administration. However, safety protocols are still being developed, and this should only be done under physician supervision with appropriate maternal screening for infectious agents.
6. Optimize Complementary Feeding When the Time Comes
The transition to solid foods is another critical window. The review notes that complementary feeding practices influenced constipation outcomes independently of delivery mode. A diverse, fiber-rich diet that supports ongoing microbial development is foundational. Fermented foods appropriate to age, diverse plant foods, and minimizing early processed food exposure all support the microbial flourishing that C-section birth may have delayed.
Dr. Jill’s Clinical Perspective: I tell my patients what I would tell a dear friend: if you have had a C-section, or if you are planning one, you have not failed your baby. You have made a decision (or had a decision made for you) that was right for your circumstances. But now you have knowledge. And with knowledge comes agency. Breastfeed if you can. Supplement wisely with synbiotics. Limit antibiotic exposure. Hold your baby skin-to-skin. Feed them the rainbow of vegetables and fiber-rich foods when the time comes. These are not small acts. These are profound, scientifically-supported investments in a future of health rather than chronic disease.

A Word from Dr. Jill: On Healing, Hope, and the Wisdom of the Body
Science is one of the great gifts we have been given. The ability to peer into the molecular world of a newborn’s gut and understand what is happening there, to connect the dots between how a baby enters the world and whether they develop Crohn’s disease or food allergies twenty years later, is extraordinary. It humbles me.
But science is not the whole story. I have walked my own road through gut disease, through Crohn’s, through toxic mold illness, through my own reckonings with a body that has challenged me in ways I never anticipated. And what I know now, deeply and personally, is that the body has an astonishing capacity to heal when we give it what it needs.
The microbiome is not fixed at birth. It is not a sentence. It is a living ecosystem, responsive and resilient, that continues to be shaped by every meal we eat, every relationship we cultivate, every breath of clean air or exposure to toxin. The dysbiosis that begins with a C-section delivery is real and meaningful. And so is the potential for restoration.
I pray for every parent reading this that you would hold both truths at once: the seriousness of the science and the enormity of the healing that is possible. That you would approach your child’s health not with fear, but with the kind of informed, empowered love that says: I see what happened here, and I am going to do everything in my power to support this little body toward wholeness.
That is root-cause medicine. That is what we do here.
Connect with Dr. Jill
- www.jillcarnahan.com
- www.drjillhealth.com
- Podcast: Resiliency Radio (YouTube, Spotify, Apple Podcasts)
- Unexpected: Finding Resilience through Functional Medicine, Science, and Faith
If you found this article helpful, share it with a new parent in your life. Early knowledge is early healing.
Scientific References
- Al-Beltagi M, et al. Gastrointestinal consequences of cesarean section birth: A systematic review of short- and long-term effects in infancy and beyond. World J Clin Pediatr 2026; 15(1): 111501. DOI: 10.5409/wjcp.v15.i1.111501
- Salvatore S, et al. Neonatal Antibiotics and Prematurity Are Associated with an Increased Risk of Functional Gastrointestinal Disorders in the First Year of Life. J Pediatr 2019; 212: 44-51.
- Shao Y, et al. Stunted microbiota and opportunistic pathogen colonization in caesarean-section birth. Nature 2019; 574: 117-121.
- Dahlen HG, et al. Gastro-oesophageal reflux: a mixed methods study of infants admitted to hospital in the first 12 months following birth in NSW (2000-2011). BMC Pediatr 2018; 18: 30.
- Nakamura M, et al. Association of cesarean birth with prevalence of functional constipation in toddlers at 3 years of age: results from the Japan Environment and Children’s Study (JECS). BMC Pediatr 2021; 21: 419.
- Bager P, Simonsen J, Nielsen NM, Frisch M. Cesarean section and offspring’s risk of inflammatory bowel disease: a national cohort study. Inflamm Bowel Dis 2012; 18: 857-862.
- Hellsing C, et al. Delivery mode and risk of gastrointestinal disease in the offspring. Acta Obstet Gynecol Scand 2022; 101: 1146-1152.
- Andersen V, et al. Caesarean Delivery and Risk of Chronic Inflammatory Diseases: A Population Based Registry Study of 2,699,479 Births in Denmark. Clin Epidemiol 2020; 12: 287-293.
- Mitselou N, et al. Cesarean delivery, preterm birth, and risk of food allergy: Nationwide Swedish cohort study of more than 1 million children. J Allergy Clin Immunol 2018; 142: 1510-1514.
- Kuitunen M, et al. Probiotics prevent IgE-associated allergy until age 5 years in cesarean-delivered children. J Allergy Clin Immunol 2009; 123: 335-341.
- Wang Y, et al. Restoration of gut microbiota with a specific synbiotic-containing infant formula in healthy Chinese infants born by cesarean section. Eur J Clin Nutr 2025; 79: 567-575.
- Dominguez-Bello MG, et al. Delivery mode shapes the acquisition and structure of the initial microbiota across multiple body habitats in newborns. Proc Natl Acad Sci USA 2010; 107: 11971-11975.
* These statements have not been evaluated by the Food and Drug Administration. The products mentioned in this article are not intended to diagnose, treat, cure, or prevent any disease. The information in this article is not intended to replace any recommendations or relationship with your physician. Please consult with a qualified healthcare provider regarding any health concerns for yourself or your child. Individual results may vary.
© 2026 Dr. Jill Carnahan, MD | Flatiron Functional Medicine | 400 S. McCaslin Blvd, Suite 210, Louisville, Colorado 80027 | www.jillcarnahan.com | www.drjillhealth.com








Share: