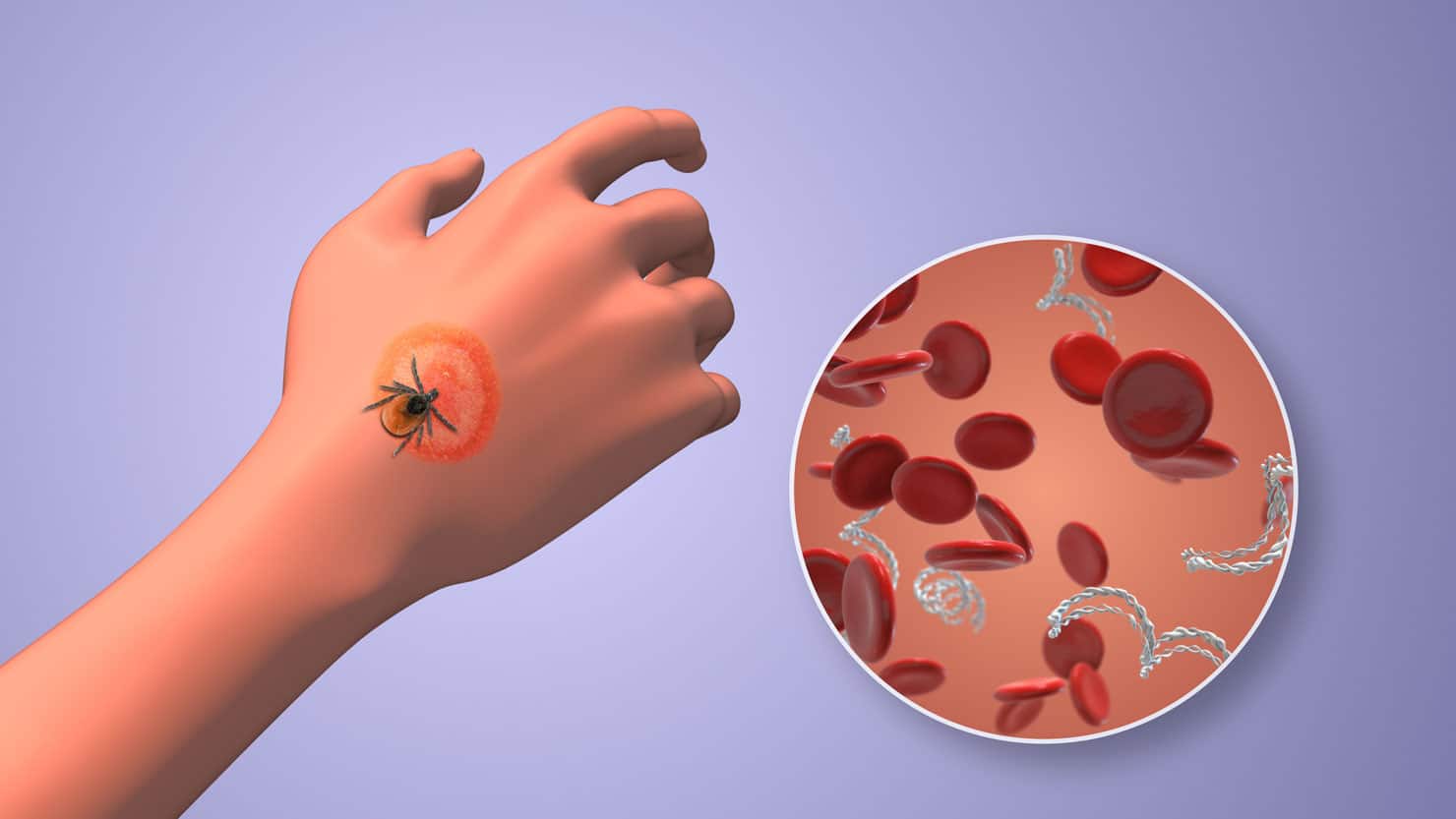
In Episode #67, Dr. Jill interviews Dr. Ann Corson about issues with hypercoagulation in chronic illness, and how Inflammation and infection may cause excess fibrin production. Excess fibrin production impairs oxygen getting to tissues and vital organs.
Key Points
- Inflammation and infection can cause excess fibrin production
- Excess fibrin production can cause layer that impairs oxygen getting to tissues and organs and causes many symptoms including local hypoxia, fatigue, exercise intolerance
- Platelet dysfunction is also very common after Lyme disease, mold toxicity or other infection or inflammatory process.
Our Guest – Ann Corson
Dr. Jill
Dr. Jill Carnahan is Your Functional Medicine Expert® dually board certified in Family Medicine for ten years and in Integrative Holistic Medicine since 2015. She is the Medical Director of Flatiron Functional Medicine, a widely sought-after practice with a broad range of clinical services including functional medical protocols, nutritional consultations, chiropractic therapy, naturopathic medicine, acupuncture, and massage therapy. As a survivor of breast cancer, Crohn’s disease, and toxic mold illness she brings a unique perspective to treating patients in the midst of complex and chronic illness. Her clinic specializes in searching for the underlying triggers that contribute to illness through cutting-edge lab testing and tailoring the intervention to specific needs.
Featured in Shape Magazine, Parade, Forbes, MindBodyGreen, First for Women, Townsend Newsletter, and The Huffington Post as well as seen on NBC News and Health segments with Joan Lunden, Dr. Jill is a media must-have. Her YouTube channel and podcast features live interviews with the healthcare world’s most respected names.
A popular inspirational speaker and prolific writer, she shares her knowledge of hope, health, and healing live on stage and through newsletters, articles, books, and social media posts! People relate to Dr. Jill’s science-backed opinions delivered with authenticity, love and humor. She is known for inspiring her audience to thrive even in the midst of difficulties.
The Podcast
The Video
The Transcript
#67: Dr. Jill Interviews Dr. Ann Corson on “What’s the Fuss about Fibrin?”
Dr. Jill 00:13
Okay, it looks like we're live, everybody! You are in for such a special treat today! I'm here with Dr. Corson and I'm going to introduce her in just a moment here. She's a wonderful guest. We haven't known each other that long, although we've been in the same circles for years. So I've known of her and have had the greatest respect for her work and the lectures she's just given recently about fibrin. We're going to dive into that in just a minute or two. But before we do, I want to give you just a little background.
Dr. Jill 00:41
You all know me. You've been here before. If you want any of the past interviews, you can see everything that I've recorded on my YouTube channel. It's all free and there's like 60+ hours of interviews with great experts like Dr. Corson here. It's on my YouTube channel under my name, Jill Carnahan. If you do go there and enjoy them, please subscribe so you stay updated on the new content. And this video, depending on where you're watching it, will either land on YouTube in a week or so or maybe you're watching it live. Other background: If you want other information on blogs or things on my website, it's just JillCarnahan.com. And I don't often mention products, but if we do, you can find those on DrJillHealth.com.
Dr. Jill 01:22
I am absolutely delighted to introduce Dr. Ann Foulke Corson. She grew up in southeastern Pennsylvania and obtained a Doctor of Medicine degree in 1982 from the University of Pennsylvania School of Medicine in Philadelphia. She's been board-certified in family medicine—just like me—since 1983 and integrative holistic medicine. So we have the same credentials too. Integrative family medicine is a unique field that combines modern Western medical science, traditional herbal medicines, and nutrition as informed by the philosophies of ancient Chinese medicine. And again, we practice very similarly too.
Dr. Jill 01:57
I'm sure what Dr. Corson and I both have seen is that we have this wonderful foundation of Western science, but then it's like our toolbox is bigger now that we're able to use all these other modalities as well to help people. And I don't know about you, Dr. Corson, but I find we need those tools, right? We need everything possible nowadays with a complex chronic illness.
Dr. Jill 02:18
She approaches environmental, infectious, dietary, metabolic, biochemical, endocrine, immunological, structural, emotional, and spiritual detriments to disease. Her practice focuses on identifying and addressing the root cause of each patient's illness. She has a solo practice in Philadelphia and we were both just saying before we got on here how, gosh, the patients are coming out of woodwork. It's really hard to keep up. I think that as COVID hit, people packed away. They're starting to come back out and realize how important health is. We're both just realizing the need to educate. And one of the things you'll find today, whether you're a clinician listening or a patient, [is that] this information is really, really important. She has so many awards and credentials. She's been speaking around the world. I won't read the rest of this here, but you can find her. And your website, Dr. Corson? Where can they find you?
Dr. Ann Corson 03:11
AnnFCorsonMD.com. It's a very rudimentary website, so don't expect much from it at all.
Dr. Jill 03:20
That's okay. Well, we are so delighted to have you here. So welcome, and thanks for coming. And before we jump into the fuss about fibrin, what this is all about, and why it's so important to the people listening—if you're a practitioner or patient—I would love to hear just a little bit about your journey. It's very, very parallel to mine with family medicine and then the holistic integrative. How did you get into medicine? And how did you get into integrative medicine? Tell us a little about your story.
Dr. Ann Corson 03:44
Well, I come from a long line of doctors. And for some reason, my siblings knew it was always me who was going to be the doctor, although at first, I thought I was going to be a neuroanatomist. So I sort of rebelled and went to graduate school in neuroanatomy before turning around to go to medical school. But I just seemed to fall into that naturally. The nervous system was my first love, so I was thinking [of doing] neurology or something like that. I started out that way, but then I really found that that was very limiting. So I actually became an emergency physician, and I practiced emergency medicine for close to 15 years—not quite.
Dr. Ann Corson 04:23
Then my only child got quite ill, and it took me a couple of years to figure out what it was. I remember complaining to a friend of mine one day, “I can't figure out what's wrong with him.” And he said: “Well, he's got Lyme disease. Look at the symptoms.” I said, “Well, I've done the ELISA [test] three times and it has come out negative.” That's what the American Academy of Family Medicine always tells us to do. So he gave me a flyer for a lecture that Dr. Joe Burrascano was giving on the 3rd of May or the 8th of May—I can't remember quite—2003 at the local high school here in Chester County, Pennsylvania. I went and I was just so enthralled. I learned more in that lecture than I had in years of going to medical meetings and whatnot. So I realized that my son had Lyme disease in 2003.
Dr. Ann Corson 05:20
Just a short time after that lecture, I asked Burrascano if I could come visit him in his office, because that's the way we learn things in medicine—see one, do one, teach one. So you have to learn. He said: “Well, that's okay. No one has ever done that.” I started the whole physician training program with ILADS because I was the first one to ever ask. And he said, “But you know, next week I got somebody coming from Wales.” David Owens came the next week, so I spent time learning with him. I went first in July and then went back in September of '03.
Dr. Ann Corson 05:52
A couple of years later, I went and trained with Charles Ray Jones in Connecticut. But man, I just hit the floor running in the summer of 2003 with Lyme disease and just started my own treatment. I've been an ER doctor and I've done primary care in family practice offices and workman's compensation situations. I've helped in the OR. I worked in the ER. So I had a lot of primary care clinical experience, but I found that these were the most complicated patients you could imagine.
Dr. Ann Corson 06:21
Then, in 2004, there was a local psychiatrist by the name of James Schaller who was sharing patients with me. He said, “We also have a mold problem, Ann.” I said, “What do you mean?” So he gave me a pre-print copy of Mold Warriors. So I heard about mold in 2004. I started treating mold in 2004. Then I had a patient come to me and she put a bottle of Toxex on my desk, which is a Pekana product. She said, “I don't know what this stuff is, but this is really good s___.” She says, “I took two drops of it and I was sick for a day and a half.” So I said, “I've got to look this up.” I looked up the company and I started exploring all of these natural remedies.
Dr. Ann Corson 07:06
I learned about German biological medicine. I also just jumped right into the deep end. I went to all these trainings by Gary and Rain Klepper and some of these other people and got into sort of that northern California naturopath community. And I just found my tribe, you know. That was in 2005. So I learned about hypercoagulability way, way back in 2005, from Gary Klepper, who learned it from David Berg a couple of years prior. So again, I just hit the floor running and kept going. And I've just found a wonderful armamentarium of medicine and things to use for my patients, and I have been growing and growing and growing all these years. It's just been a blast because it's so much fun to help whole families get better.
Dr. Jill 07:53
Oh, what a beautiful journey! And it's so driven, same as my journey, by this inquiring and curiosity, right? Again, we've got a great training background. I have all the respect in the world for our allopathic training and medical school and yet, we ran into limitations in our own lives and it's like: “What else is possible? And then, “What else is out there?” Then we start to realize, “Oh, there's a whole other world of ability to treat and help.” And I feel like it's the best way to really combine Western allopathic medicine with all of these other things. Like you, I learned so much from my naturopathic friends.
Dr. Jill 08:28
So hypercoagulability—let's first define it. But I just want to say [something about] my personal experience. I've known about this. I've known how it correlates with Lyme and complex chronic illnesses like mold and COVID. So I want you to describe a little bit about: What does that mean for people who are lay persons, fibrin and hyper-coagulability? But I will say, I felt like this is one of those missing links in a lot of practitioners' toolboxes to understand how much this affects so many of their chronic patients.
Dr. Ann Corson 08:58
It's so true because the issue of hypercoagulability is often overlooked, even by the most experienced integrative practitioners. People will often come to me after being to many people that I respect greatly and it's one of the things that has not been looked at at all. But unfortunately, it's really present to some degree or another in almost every chronically ill patient, and it's present in acutely ill patients as well. So think about it: Everyone has had the flu, right? Everyone has had a fever, a headache, body aches and pains, fatigue, nausea, and insomnia, right? A lot of those symptoms can be exacerbated by the hypercoagulability that happens when there's any inflammation in the body.
Dr. Ann Corson 09:37
An acute inflammatory response from a flu also drives the hypercoagulable fibrin-producing response in the body. So whenever we acquire it, we have a brisk innate immune system response. Then part of that innate immune system response activates the coagulation cascade, which is this domino effect where the body creates more soluble fibrin. So a lot of these symptoms can be attributed to that. And acute or chronic innate immune system activation [from] heavy metal toxins, mold toxins, chronic mast cell activation, Herxheimer reactions, or inflammation of any kind can result in the generation of excess soluble fibrin.
Dr. Ann Corson 10:27
So what's hyper-coagulability? Well, the body maintains this wonderful balance—this seesaw balance [and] a very delicate balance; it's very redundant—of proteins that either encourage or discourage blood clotting. This is a very, very complex and redundant system. And it's very, very important because, after the injury to a blood vessel, we need to be able to immediately plug and stop that bleeding. But we also have to stop the formation of that clot so that we don't make so many clots that we block that blood vessel and damage tissues. You'll have to excuse me; I'm in the middle of a big thunderstorm here, so if I get interference in my internet connection… I'm on an Ethernet cable, so hopefully it will be all right.
Dr. Ann Corson 11:12
So you've got to be able to either plug or thin, clot or unclot all the time. Now, when this delicate seesaw is in balance due to a genetic factor, an environmental factor, a toxin infection, emotional stress, or physical stress—like physical trauma, surgery, or something like that—then it can result in too much soluble fibrin being made and not being able to degrade it enough. So if you can't degrade it enough, you end up being “sticky.” And that's sort of the sticky side. So you have an abundance of molecules that are encouraging the formation of fibrin and blood clotting over blood thinning. So these are many different causes that can precipitate us into it.
Dr. Ann Corson 12:03
Well, what is soluble fibrin? The coagulation cascade proteins are a series of molecular reactions that result in the production of fibrin. Fibrin molecules can either be soluble and free-floating in the bloodstream or they can become insoluble and cross-linked and that creates a clot. It takes a burst of thrombin to actually cross-link them to make them a clot. They're kind of like interlocking Lego toy pieces. Okay, that's the clot. But generally, in the absence of a tear in a blood vessel wall, you don't actually get that cross-linking happening—that burst of local thrombin that causes the interlocking. So you generally just get excessive soluble fibrin produced right in the area, and that creates a sludgy layer on the surface of the endothelial lining of the blood vessels.
Dr. Ann Corson 13:01
Just one micron, which is one-millionth of a meter thick, of a layer of soluble fibrin along the inner lining of the capillary reduces the diffusion of oxygen molecules out of the blood into the tissues by 500%, with resulting tissue hypoxia. And that was referenced. Nemerson had given a lecture at a 2003 meeting. I can't find the original article, but I can give you the information about Dr. Nemerson. But Dr. David Berg references this in a lot of his lectures that he gave over the years about hypercoagulability. And there's a wonderful picture of the capillary, which we can show if you'd like. So even a small amount of soluble fibrin in the bloodstream and that sludging can create very significant clinical symptoms. And most allopathic medicine doesn't even think about it until you've got a blood clot like a DVT [inaudible].
Dr. Jill 13:59
Right. Let's talk briefly about the symptoms. What would a patient look like if they had an issue with this? And it's probably going to be very non-specific, right?
Dr. Ann Corson 14:12
Right. And then after that, I'd like to talk about the different ways the body deals with coagulation because, especially in our current era, we need to think about platelets as well as fibrin formation. So the signs and symptoms of hypercoagulability: If you wake up in the morning and you're stiff all over your body, or if you've been sitting for a while and you get up and you feel stiff. If you're nauseated upon awakening or if your appetite's very poor in the morning. Sometimes painful teeth or a sensation of the teeth being loose. Having very poor aerobic exercise tolerance where you have post-exertional fatigue, shortness of breath with exercise, and exacerbation of pain with exercise, or your muscles just get so painful. If you have fatigue and issues with insomnia. Let me just see if I'm missing anything. Brain fog and irritability. Anxiety is a big, huge one. I often treat hypercoagulability with anxiety with fibrinolytic enzymes. You can have depression. You can have mood swings and fatigue. Generalized pain that could be utterly debilitating, kind of like: “I just hurt everywhere. Every time you touch me, I hurt,” because the tissues are hypoxic. You can have painful numbness or pins and needles, sharp stabbing, shooting pains, and deep aching pains, especially in the arms and legs. You have limbs that fall asleep really easily, or an inability to, as I say, tolerate aerobic exercise with worsening pain and fatigue after exercise. Insomnia can be included in that, as well as restless legs. When you're laying down, trying to go to sleep at night and you just can't get comfortable and you've just got ants in your pants and you're restless and your legs just can't get comfortable, often that's hypercoagulability at night. So those are the major symptoms that people will have with it.
Dr. Jill 16:24
What about headaches and migraines? Would you put those in that class? Or not necessarily?
Dr. Ann Corson 16:28
[inaudible] they can. It is very good to add that, especially with some of the side effects that people are now seeing after being vaccinated. Headaches and migraines can be a sign of sludging as well as serious clotting in the brain vasculature. So yes, thank you for adding that.
Dr. Jill 16:51
Good. So you talked about fibrin. You got the sticky blood. You gave symptoms and that would probably include this whole hypercoagulability hypoxic thing. And then you want to go onto platelets. I kind of interrupted you.
Dr. Ann Corson 17:02
What I'd like to do is talk about what the physical signs are because people can see these in themselves as well as the clinicians who are listening can see them in their patients. So you know how people sometimes get mottled skin when they're cold? We especially see that in babies and infants. Well, people who have chronically mottled skin may be hypercoagulable. They have cold, clammy extremities, but they're essentially warm. They have very prolonged capillary refills in their fingers and toes. They can have a very pale, swollen tongue with scalping of the tongue edges from indentation from the teeth. That's not just hypothyroidism. That can also be splenic congestion or hypercoagulability.
Dr. Ann Corson 17:45
You can have a very doughy abdomen when you examine someone's abdomen with periombilical fullness and tenderness. And you can see generalized soft tissue congestion, as if the tissues are just sort of boggy. They say, “Well, it's like I used to be able to see my tendons in my hands and now I can't even see them anymore.” Often, the head neck can be very red or ruddy in color upon lying down. Then the feet when people are sitting can be really purple when they're sitting on the exam table and their feet are just hanging. There's often a very significant compromise of cognitive function, not only with irritability but [also with] emotional lability.
Dr. Jill 18:28
Excellent. Yes, I'm sure a lot of you are listening, whether you're a clinician or patient, and are resonating, especially if you've dealt with Lyme and mold. I really think, like I said, Dr. Corson, this is such an important piece for many, many of our chronic patients. And I mentioned COVID, but any virus, especially an inflammatory virus like COVID, can also be in this pathway, correct?
Dr. Ann Corson 18:49
Yes, that's correct. It doesn't have to be, but we'll talk about that a little bit later. I don't want to get into it yet. Okay, so now, how does the blood coagulate? There are three main mechanisms. Number one, if your platelet behavior and whether platelets have been activated to clump… And that's separate from the protein cascades that either make fibrin or break down fibrin. So it's platelet behavior, fibrin formation, and fibrin degradation. Those are the three main mechanisms that are controlling it. Now, platelets will aggregate and stick in response to trauma to the blood vessels in response to immune system activation by toxins or infections. And one of the problems with the spike protein is that it activates platelets. It also damages the endothelial lining. That also stimulates the coagulation cascade.
Dr. Ann Corson 19:44
So you've got two things you have to think about in this scenario now: What we're currently dealing with with the spike protein, both in natural infection and vaccination, is not only platelet activation [but] also fibrin formation. So the treatment for that is going to be a little bit different than what we would do for just someone who's got hypercoagulability from mold toxins, metal toxins, or some other issue. So again, there's always this physiological balance between formation and degradation. Normally, platelet aggregation is pretty easy to deal with. You normally use high-dose essential fatty acids, vitamin D, and sometimes baby aspirin and things like that. Usually, you think of platelets as being pretty easy to deal with, but [considering] the intensity with which the platelets aggregate given our current issues that we're dealing with in our country, we have to be very, very aggressive about that. We have to buffer both the fibrin formation and platelet activation.
Dr. Jill 20:52
Are you recommending anti-platelet therapy for patients who've either had long-haul COVID or post-vaccination issues?
Dr. Ann Corson 21:01
Yes, but primarily very high-dose essential fatty acids. I usually try to get between three and four grams a day of a very pure omega-3, at least 400 international units of vitamin E, and depending on their symptomatology and what else they need, maybe a baby aspirin a day. You really have to block platelet activation.
Dr. Ann Corson 21:26
Unfortunately, for the blood tests that we do to evaluate coagulation, we used to be able to get platelet activation testing but when Esoterix was bought by Labcorp, they dropped that test. So initially, David Berg had set up HEMEX, and then Esoterix bought it and then Labcorp bought Esoterix. So, you can get these tests all through Labcorp, but they dropped the ones that indicated whether the platelets had been activated. That's a real problem because nowadays, we really need to know [inaudible].
Dr. Jill 21:56
We need it, right? I've noticed that too. It's hard to get the information that we need.
Dr. Ann Corson 22:00
Yes, it's very hard. You can get information about your fibrin formation and degradation and your thrombin formation and degradation, and you can get some clues as to the genetic issues that people have. But it's very difficult to get information about platelets, so it's safer to treat them as if their platelets are going to be activated.
Dr. Jill 22:22
Quick question on that because, with Crohn's, colitis, or some inflammatory disorders, we see thrombocytosis—which, for those of you who don't know, is excess platelet production, not necessarily how they behave. Would just thrombocytosis alone also contribute to issues or would it have to be the activation of those excessive platelets?
Dr. Ann Corson 22:40
No, whenever you've got too many cells—of course, it depends on how high you get—you can get all kinds of sludging and blockage. Yes. Just when you have abnormally shaped red blood cells in sickle cell anemia or you have Babesia and you have some other red blood cell inclusion and the red blood cells can't squeeze through the capillary beds, you're going to have some problems. So, we talked about the symptoms of hypercoagulability. We talked about the physical signs of hypercoagulability. Again, a good way to start dealing with it is to really help with your omega-3-to-6 ratio. Most people in this country need very high doses of omega-3s for a prolonged period of time. You really need to optimize your liver detoxification pathways, but you're not going to do that until you fix your gut dysbiosis.
Dr. Ann Corson 23:36
And what I'm finding is that [with] the vast majority of people—at least in this part of the country where we have a great deal of glyphosate used in our agricultural areas all around southeastern Pennsylvania—their lactobacillus has been totally wiped out. It's just not growing at all in their stool tests. So, we need to make sure that we are fixing that gut dysbiosis by trying to restore the lactobacillus. The best way to do that so far, I'm finding, is to have as clean a diet as possible to bind and get rid of the glyphosate that you have in your body. You have to replace the manganese and other trace minerals because manganese is very essential for lactobacillus to grow. And then I use a very high-dose lactobacillus in order to try to replace that along with your normal prebiotic, so whatever you like to use, for gut dysbiosis.
Dr. Jill 24:34
Yes. For listeners who don't know, glyphosate was originally just a mineral chelator, and they found it to have this anti-herbicide effect. But the minerals it chelates are also in our gut. So, when they do the studies on the cells, they're like, “Oh, there's no problem,” but it has a massively profound detrimental effect on our gut because it preferentially will chelate those minerals that our lactobacillus, bifidobacteria, and probiotics need to survive. So, thanks for mentioning that, because I see that all the time as well.
Dr. Ann Corson 25:02
Yes, and it's really horrible. To try to reverse it can be a difficult and long process. So you really have to deal with that because, as long as you've got all this toxic dysbiosis in the gut, you're going to have all this nasty stuff heading up into the liver. And it's hard to normalize your liver phase I, phase II, and all your detoxification if all this nasty stuff keeps going up every time you eat. So, you really have to start with the gut, and that will help to reduce the inflammation in the body and lower your risk of hypercoagulable responses to things because the lower your overall systemic inflammation, the easier it's going to be for you to weather these kinds of stresses that you come across. And again, cleaning up your extracellular matrix space—that's the fluid that bathes every cell in the body with this pulsatile movement that comes from the primary respiratory mechanism eight times to ten times a minute. That just bathes and soothes every cell in the body. The best way to do that is to make sure you have adequate cleaning up of your lymphatic fluid, your blood, your kidneys, and your liver of any of the drainage medicines that you prefer. Clean eating is the best thing that you can do.
Dr. Ann Corson 26:16
So these are the things [you can do]: [Get] adequate antioxidants, supplements that you may need, appropriate physical exercise, keep your blood moving, and [practice] stress reduction. We're all living in a time where, unfortunately, a lot of people are very caught in that fear cycle. And if you're caught in that fear cycle, you're going to have really increased cortisol levels. That in and of itself can create hypercoagulability. So you have to learn to let go of your fear. You have to step away from this psyop that we're being exposed to and realize that you can have control over your life and your family's life and start taking positive steps. And I do believe that having some connection to a higher power in a spiritual way, putting your faith in that higher power, and realizing that good always triumphs over evil [are important]. And it's just going to take a certain tipping point for humanity to realize that they have to change the side of good before things are really going to change.
Dr. Jill 27:26
I love that you mentioned that. We know the physical and we know all these things. But with these complex chronic patients that we both see, I always want to make sure that they have some sort of connection to a higher power or whatever their belief system is, and that there is hope. If you're watching the news for one, it gets so heavy. So encouraging people to think on a little bit of a different plane can be really helpful; otherwise, it's dark and dreary.
Dr. Ann Corson 27:59
Yes. You have to turn off mainstream media because most of it is propaganda anyway. So you can't allow that fear [to be] driven because you're never going to get better until you do that. Many years ago, I was exposed to the practice of Falun Dotha. Falun Dafa is a meditation system of mind and body where, as you improve your moral character and do simple exercises, you ascend spiritually. It began in 1999 in China and spread all over the world. So if you align with the basic truths that support everything in the universe—number one being truth, number two being compassion, and number three being tolerance and forbearance—the closer we align with those and the more we understand that those will always prevail over anything negative, then we can always have hope and ascend to a higher level. And that's the way you get better, because so much of your illness really comes from your emotional and psychological state.
Dr. Jill 29:10
Yes. So what else do we have on… So we talked about fibrin and we talked about platelets. We talked about the symptoms clinically.
Dr. Ann Corson 29:18
Let's see what else I wanted to talk about.
Dr. Jill 29:21
And we can talk about treatment, for sure. We talked just briefly about platelets, but you may want to…
Dr. Ann Corson 29:28
Yes. Again, let's talk about some of the consequences that happen when you have excessive soluble fibrin in the blood vessels and why it's such an issue. If you have the sludge that's lining the blood vessel, number one, you can't get oxygen out. You also can't get nutrients out. You also can't get wastes back in for elimination. And the lymphatics out in the tissues get all congested; they can't dump stuff, and they get sticky. So you've got intravascular (inside the blood vessels) and extravascular (outside the blood vessels) spaces that are compromised, stuck, swollen, and can't move things. It can't move toxins. It can't move nutrients, vitamins, growth factors, or necessary minerals. So you get organ and tissue compromise and that's why you have a lot of these symptomatologies because the brain, especially, is very compromised. Also, when the vessels have that sludge, they become rigid and they can't respond to the autonomic nervous system's constriction or dilation orders that the autonomic nervous system is always giving.
Dr. Ann Corson 30:46
So what happens when you have rigid blood vessels? You have alterations in your autonomic responses and control of blood pressure. So either these people have high blood pressure, they have difficulty controlling it, or they have what's called POTS because their blood vessels are stuck open and when they lay down, they're okay and they go to get up quickly, they faint because their blood vessels can't constrict rapidly to get blood to the head. So almost all of the patients that I see who've been diagnosed previously with postural orthostatic tachycardia syndrome are mold patients who are hypercoagulable.
Dr. Jill 31:26
Absolutely. Now, does histamine play into any of the coagulation cascade? Is there any correlation with excess mast cell stuff with this? Or are they sort of two separate issues?
Dr. Ann Corson 31:39
I think that they are. Don't ask me to tell you the biochemistry of how they're connected, because I don't know that. But mast cell activation creates inflammation. It releases a tremendous amount of cytokines. That's also going to stimulate the coagulation cascade.
Dr. Jill 31:53
That's my theory too. How? It's probably prostaglandin-related or something. But that makes perfect sense.
Dr. Ann Corson 32:01
We've been treating mast cell activation, Jill, probably for years, long before anybody called it that, because it's part of the whole syndrome of inflammation that we've been seeing for years. And there are incredibly sensitive patients who can't take anything at all. They'll explode anytime you try to do something with them, right? The other thing that I wanted to have everyone know is that when you go to treat hypercoagulability, you must take it low and slow. Let's put up one slide I have. I can hit ‘Share Screen', or do you have to do that? Okay. Let me pick what I want [inaudible]. Bingo.
Dr. Jill 32:58
There we go.
Dr. Ann Corson 32:59
Okay. It's slide 23. And I'll make sure that you have this. Okay. Now, this is the way the blood is flowing down through it. Now, this is that soluble fibrin. It's on the layer of a blood vessel wall. This is the endothelial cell here. Now, this is a really tight formation here, soluble fibrin. And you've got all kinds of things stuck in here. So when you actually go to start releasing this, all of these big bad boys, like these pathogens and toxins and things down in here, are going to be released. So you're going to have to be ready to deal with them as they're released. Also, though, what can get trapped in here is thrombin. Thrombin itself can get trapped here in this fibrin sludge layer. There's no crosslinked fibrin; it's all soluble fibrin. But it gets locked down pretty tight. So sometimes, as you go to release this, if you release it too quickly, that thrombin will cause a paradoxical dramatic increase in the amount of fibrin formation that is made. So you've got to really take your time and do this slowly. Either way, it depends on how long people have been ill, how much gunk they've got, and how many problems they have.
Dr. Ann Corson 34:40
Also, just to show you, this is the slide from the presentation from this doctor, Nemerson. And I've adapted it from one of the lectures from Dr. Berg [inaudible]. So here's the inside of the endothelial cell, the capillary bed. A red blood cell is seven microns, right? So if you've got this fibrin, which is only one micron here on the layer of the endothelial cell, it goes from two seconds for oxygen to go across in the absence of any fibrin to over five minutes if there's just one micron of fibrin there. So that's really a dramatic change in the time it takes for oxygen. And this is why people have pain in their muscles. This is why people can't exercise. There's a lot going on here. You can stop sharing now.
Dr. Jill 35:52
You can stop it and I'll check.
Dr. Ann Corson 35:54
Yes, there we go. You got it?
Dr. Jill 35:56
Yes, perfect. Okay.
Dr. Ann Corson 36:00
Not only do we have all of the mitochondrial problems because the mold toxins just stop the ribosomes in the mitochondrion, [but] the mold toxins also stop the ribosomes in all of the dividing cells. It suppresses bone marrow function and all this stuff. You also have to worry about what the hypercoaguability has done. So we've got all these different layers of problems that we have to deal with. When you go to detoxify somebody, say you're starting to detoxify mold. You're starting to take the toxins out of the body using the gut, getting them to sweat a lot if they're able to, doing a lot of glutathione, or if you're using lipids, or whatever you're doing. If you start to mobilize a lot of these stored toxins rapidly, you're going to stimulate a tremendous amount of hypercoaguable response.
Dr. Ann Corson 36:46
A lot of the Herxheimer reactions are in people getting hypercoaguable. The same thing with heavy metals. Heavy metals are just really bad boy toxins. As you start to mobilize them from where they're stored in the matrix out in tissues and then move them through the bloodstream to the liver and out, you are going to have a lot of issues with coagulation being stimulated by those bad toxins as they're going through the bloodstream. That's why whenever you are treating Herxheimer reactions, you need to include enzymes, and not just fibrinolytic enzymes but also often proteases.
Dr. Jill 37:26.
Uh-huh. Proteolytic. We have about a good 10 minutes left. Let's maybe go a little bit to treatments and what we can do about this. This is so fascinating. And really, it's covering such a spectrum of our patients. I mean, I wonder if there is a patient that doesn't have some issue with this, because it's inflammation, infection, and toxin related. And I think that's all of my population.
Dr. Ann Corson 37:53
I think almost all of my patients are on some kind of enzyme. That's the hole that I see in the vast majority of the patients that come to me from other practitioners.
Dr. Jill 38:05
I agree. Again, I'm so glad to have you here and your expertise. I have been doing this for 20 years, and there are many, many, many of our colleagues that don't really treat or understand this piece of it. And it's critical—absolutely critical.
Dr. Ann Corson 38:18
Yes, it really is. So there are two main fibrinolytic enzymes. One is nattokinase, and the other is lumbrokinase. And unfortunately, there are many brands out there, but there are only a few that really work. And I don't know whether you want me to name those, or not name those, or tell you—
Dr. Jill 38:37
Let's do it because this is all commercially free. It doesn't matter; we can say whatever we want.
Dr. Ann Corson 38:42
And I have no commercial arrangements with these companies at all. Really, I was taught this by Gary Klepper years ago, and he's right. The nattokinase from Allergy Research Group, the soft gels—they have a 36, and they have 100. I think they're discontinuing the 36. I wish they wouldn't.
Dr. Jill 39:04
Yes, [inaudible] start people on that low dose, isn't it?
Dr. Ann Corson 39:08
Yes. Especially with the kids, sometimes it's better. They, for some reason, are more effective. And I don't know whether it's the way that that softgel is dissolved lower in the gastrointestinal tract or not. But any of those nattokinases that come in capsules are just not worth their time. Now, there are some kids who have been too young to swallow, even the small little football of nattokinase. So I'll sometimes use a combination Natto-Serrazime or something like that, from like Designs for Health, or I'll use a capsule one in apple sauce, but using a much higher dose and hoping that I get it through the stomach—at least enough. Of the lumbrokinases, I'm terribly sorry, but only the Canada RNA brand name Boluoke works.
Dr. Jill 39:58
Yes, agreed. Totally. It's the only one I would do.
Dr. Ann Corson 40:01
And I've been doing this for a long time. I started treating hypercoagulability in 2005, which is 16 years ago. And I've had it substantiated. I have a patient in England who tried it because it was hard to get. She tried both the Doctor's Best and the Allergy Research Group lumbrokinases. And she goes to see a good cranial osteopath. Well, each time she went off the brand name Boluoke and went to one of these other brands, the osteopath would say, “Your mechanism is all sticky. This is bad.” So I've had other people substantiate it. That's not the only example, but I've had other substantiation of the fact that that one particular Japanese-made Boluoke is the only one that really works.
Dr. Ann Corson 40:48
So think about, well, how do they work? The nattokinase works primarily inside blood cells. So that's going to be really helpful now with the problems that we have with spike protein damaging endothelial cells. The Boluoke works both inside and outside the blood vessels. And it is said to be significantly stronger. I don't know. There are times when, for me, nattokinase tends to work best. And sometimes I use just Boluoke. Sometimes I use both of them at the same time. The Boluoke—only about 10% of it is said to be absorbed through the gut. So I gave both of these on an empty stomach. Way back, Klepper taught that these are hard on the gut. I rarely see anybody having any trouble taking them on an empty stomach.
Dr. Jill 41:34
I would agree that I've not had any issues and I have a lot of patients with gut issues.
Dr. Ann Corson 41:40
Yes. And then people always wigged out, “Well, I don't know; the nattokinase is dry from soy.” Well, there's so little of any kind of soy protein in the nattokinase. I have not had any problems with people who are anaphylactically allergic to soy, not having trouble with the nattokinase from the Allergy Research Group. I just haven't. I was worried about it. I say, “I'd really like you to just give it a try.” And they just haven't had problems with it.
Dr. Ann Corson 42:07
Now, there are other serrapeptidases. There are really good—lots and lots of different brands of serrapeptidases and things and things that you can use for hypercoagualability. One that I really like is imported by Marco Pharma in Oregon; it's called MarcoZyme. It's got some bromelain and other things in it. But for me, taking high doses of that several times a day for people who have been exposed to COVID, who have been exposed to vaccinated people who are now worried about transmission of the spike protein to them—that shedding of the spike protein that a lot of us are worried about—or the actual people who got the vaccine itself who realized that maybe they did something they shouldn't have done, the MarcoZymes seem to help to break up that spike protein as it's circulating if it's in the bloodstream. I don't have any proof of that. This is a purely clinical observation. And it's only one doctor's experience, so you really have to take it with a grain of salt. But that seems to be helpful.
Dr. Ann Corson 43:14
Now, sometimes, you need to use heparin. And I've found that either the subcutaneous Lovenox or an intravenous heparin has always been far superior to any of the sublinguals. I know that some of the naturopaths like the sublinguals because they don't have access in many states to injectable medications; in some states, they do. Then there are a lot of other homeopathic herbs that work. Of course, I talked about the omega fats helping—and they also help the blood vessels—the vitamin E, the phospholipids. The phospholipids can be incredibly healing to the blood vessels and the endothelial lining. As well as certain herbs. There are herbs that help. Danshen is a wonderful herb that helps with the coagulation issues.
Dr. Ann Corson 44:03
So these are all things that you can use, as well as things such as a clean diet, lowering their insulin resistance, fixing their gut dysbiosis, fixing liver detoxification pathways, adequately hydrating themselves, appropriate exercising, reducing stress and all those things. Now, there are other herbs that can help. Ginkgo can sometimes help. Other anti-inflammatory and antioxidant types of herbs can help. There are so many that it's not worth trying to name them.
Dr. Ann Corson 44:40
Now, again, if the platelets are really activated, then I would use an 81-milligram baby aspirin a day with high-dose essential fatty acids. Now, some of the caveats to that are that if someone has to undergo surgery, you really need to stop your omegas, your vitamin E, and your aspirin, or NSAIDs, a good two weeks prior to surgery. And you can restart them as soon as there's hemostasis after surgery, like 48 hours if there's no bleeding. Or, usually, like with wisdom teeth extraction, you wait until all of the oozing is brown in color and then they can restart those.
Dr. Ann Corson 45:19
I generally stop the fibrinolytic enzymes only 48 hours before surgery, and I have never had any problems with bleeding during surgery. Even if people have to go into surgery acutely and they're on these enzymes, then you just have to have them let the surgeon know so they may just have to hold a little longer, but they'll still clot. What's really dangerous is if their platelets are fully blocked by high-dose NSAIDs or high-dose aspirin, and that's a problem.
Dr. Jill 45:49
Yes, I totally agree. I have not had issues, and I usually just recommend patients stop before, and there's no problem at all.
Dr. Ann Corson 45:57
Yes, and they stop 48 hours before with the fibrinolytics and restart them again 48 hours later. Or if they have a drain, once the drain is removed or once the wisdom teeth drainage becomes brown, then they really don't have any trouble at all with it.
Dr. Jill 46:11
Yes. So do you keep patients on these for months, years, or forever? Or just during the acute inflammatory phase? Or what kind of time frame are they looking at?—because I found you need them in chronic issues. They often stay on them for quite a while. They feel better.
Dr. Ann Corson 46:25
Yes, quite a while. If they do have one of the genetic SNPs, one in four people is really susceptible to mold problems, and one in five are susceptible to getting hypercoagulable under stress of any kind. And the most common are: Protein S deficiencies, high lipoprotein (a), high alpha-2 anti-plasmins, and protein Cs. So if they have a significant genetic weakness, which becomes obvious when you treat them, you recheck them, and they still have a really low protein S, then you know that that's a genetic weakness. Or if they have a high PAI-1, plasminogen activator inhibitor 1, they may need to stay on fibrinolytic enzymes their whole lives. Or they may need to always know to take them during periods of any kind of stress, [such as] illness, injury, emotional stress, physical stress, [and] those kinds of things. So it just depends.
Dr. Ann Corson 47:22
Some patients will need to always be on them in order to stay healthy. When people get a mold hit, they always have to have their enzymes because they're not going to get over that as quickly as they would if they didn't use their enzymes. So healing the gut with things like Restore and using your enzymes are as important as your things to reduce inflammatory cytokines and to bind the toxins and get them out of the body. So that's always in my mold-hit protocol. So people need to understand when they use them, and that's part of what I teach my patients.
Dr. Jill 47:55
Well, Dr. Corson, this has just been loaded with such great information. And I just appreciate your work and being on here to get the information out. Like I said, this is not common—that not only our colleagues but even patients understand. And this could be one of the most important things that we're missing. I really feel like this is so critical. And just thank you for your inquisitive nature, your curiosity, your willingness to continue to learn and grow like we all do, and just for coming here and bringing this great information today. It's so, so, so important.
Dr. Ann Corson 48:28
Thank you so much for asking me. I was very honored. I've been an admirer of your work as well, so it's a mutual admiration society. We are in the same circle so to speak.
Dr. Jill 48:39
Absolutely, yes. And we all need each other. I always learn from my colleagues and friends like you, too.
Dr. Ann Corson 48:45
I am from the same tribe.
Dr. Jill 48:47
Yes. Oh, thank you. Well, thank you so much. Everybody, I know this information has been really useful. I'll be sure to include links and [I will] link to Dr. Corson's site as well. And thank you so much for joining us on this Tuesday afternoon!
* These statements have not been evaluated by the Food and Drug Administration. The product mentioned in this article are not intended to diagnose, treat, cure, or prevent any disease. The information in this article is not intended to replace any recommendations or relationship with your physician. Please review references sited at end of article for scientific support of any claims made.